


View Poll Results: What Are Your Helmet Wearing Habits?
I've never worn a bike helmet



52
10.40%
I used to wear a helmet, but have stopped



24
4.80%
I've always worn a helmet



208
41.60%
I didn't wear a helmet, but now do



126
25.20%
I sometimes wear a helmet depending on the conditions



90
18.00%
Voters: 500. You may not vote on this poll
The Helmet Thread 2
 05-17-16 | 09:07 AM
05-17-16 | 09:07 AM
#2051

Full Member
Joined: Jan 2012
Posts: 272
Likes: 36
Try 11+ years.
The poll could use an option specifically asking if a helmet thread has changed your mind.
The poll could use an option specifically asking if a helmet thread has changed your mind.
 05-17-16 | 09:51 AM
05-17-16 | 09:51 AM
#2052


Senior Member

Joined: May 2004
Posts: 12,103
Likes: 96
From: Wilmington, DE
Bikes: 2016 Hong Fu FM-079-F, 1984 Trek 660, 2005 Iron Horse Warrior Expert, 2009 Pedal Force CX1, 2016 Islabikes Beinn 20 (son's)
05-17-16 | 09:58 AM
#2053
Senior Member
Joined: Aug 2010
Posts: 588
Likes: 3
From: Southern California
Bikes: Gary Fisher Hi-Fi Deluxe, Giant Stance, Cannondale Synapse, Diamondback 8sp IGH, 1989 Merckx
joejack951:
My last post (#2050) includes several links. You'll find the answer among them.
Joe
My last post (#2050) includes several links. You'll find the answer among them.
Joe
05-17-16 | 11:14 AM
#2054
Senior Member
Joined: May 2004
Posts: 12,103
Likes: 96
From: Wilmington, DE
Bikes: 2016 Hong Fu FM-079-F, 1984 Trek 660, 2005 Iron Horse Warrior Expert, 2009 Pedal Force CX1, 2016 Islabikes Beinn 20 (son's)

Where did you find the reference to 'hard relatively flat surfaces'? Also, I'd like to see ED visits separated from actual hospitalizations as the 0-14 age group being taken to the hospital says nothing about the severity of the trauma, or indeed if any actually occurred. When you look at the stats for deaths and hospitalizations for kids and young adults, falls aren't the real issue.
Last edited by joejack951; 05-17-16 at 05:37 PM. Reason: corrected quote
05-17-16 | 01:29 PM
#2056

Senior Member
Joined: Apr 2011
Posts: 15,278
Likes: 342
From: Alpharetta, GA
Bikes: Nashbar Road
Also, I'd like to see ED visits separated from actual hospitalizations as the 0-14 age group being taken to the hospital says nothing about the severity of the trauma, or indeed if any actually occurred. When you look at the stats for deaths and hospitalizations for kids and young adults, falls aren't the real issue.
Among children ages 0 to 14 yearsDeaths: 26,085
Hospitalizations: 37,000
Emergency Department visits: 435,000
(it's a random result, there are more detailed studies available)
I think Joe is pretty much right, falls are the leading cause of TBI as I recall. I'm not going to hunt up links and argue about them but there should be enough of them to find a few that are satisfactory to you.
05-17-16 | 05:34 PM
#2057
Senior Member
Joined: May 2004
Posts: 12,103
Likes: 96
From: Wilmington, DE
Bikes: 2016 Hong Fu FM-079-F, 1984 Trek 660, 2005 Iron Horse Warrior Expert, 2009 Pedal Force CX1, 2016 Islabikes Beinn 20 (son's)
Those stats are available. Brain Injury Statistics - Brain and Spinal for example
Among children ages 0 to 14 yearsDeaths: 26,085
Hospitalizations: 37,000
Emergency Department visits: 435,000
(it's a random result, there are more detailed studies available)
I think Joe is pretty much right, falls are the leading cause of TBI as I recall. I'm not going to hunt up links and argue about them but there should be enough of them to find a few that are satisfactory to you.
Among children ages 0 to 14 yearsDeaths: 26,085
Hospitalizations: 37,000
Emergency Department visits: 435,000
(it's a random result, there are more detailed studies available)
I think Joe is pretty much right, falls are the leading cause of TBI as I recall. I'm not going to hunt up links and argue about them but there should be enough of them to find a few that are satisfactory to you.
Further, those basic stats from the CDC appear to lump 'suspected' TBI (i.e. an ED visit that didn't require any hospitalization) in with actual TBI. I haven't sat down and run all the numbers but when you look at what causes death by TBI, it isn't falls for most age groups. Which is why I suspect that simple falls aren't the issue those basic stats make them appear to be (disregarding the 65+ age group which has many other factors at play).
Last edited by joejack951; 05-17-16 at 05:37 PM.
05-17-16 | 05:55 PM
#2058
Senior Member
Joined: Aug 2010
Posts: 588
Likes: 3
From: Southern California
Bikes: Gary Fisher Hi-Fi Deluxe, Giant Stance, Cannondale Synapse, Diamondback 8sp IGH, 1989 Merckx
joejack951: This is the last time I'll respond to you.
Lookup Sophomore:
"-- We apologize in advance, but this is the actual definition: “suggestive of or resembling the traditional sophomore; intellectually pretentious, overconfident, conceited, etc., but immature."
So Long,
Joe
Lookup Sophomore:
"-- We apologize in advance, but this is the actual definition: “suggestive of or resembling the traditional sophomore; intellectually pretentious, overconfident, conceited, etc., but immature."
So Long,
Joe
05-17-16 | 06:09 PM
#2059
Senior Member
Joined: Apr 2011
Posts: 15,278
Likes: 342
From: Alpharetta, GA
Bikes: Nashbar Road
Well "hard" as opposed to "soft" is pretty much a given. Most everything causing an impact or sharp acceleration will have a surface impact. "Flat" possibly refers to sidewalks and roads which are leading locations for falls. Along with residences for which falls are mostly bathroom, may or may not be flat. Or it may be from his helmet researches which do show that impact on flat surfaces are the most likely to result in TBI. I don't know that it's worth arguing about, or the trouble to source.
05-17-16 | 06:16 PM
#2060
Senior Member

Joined: Sep 2013
Posts: 4,530
Likes: 664
From: Massachusetts
Most TBI don't require a trip to the emergency room, nor getting admitted to the hospital.
Not that this "asserted" fact will placate the anti-helmet crowd (who assert they aren't) - ever.
Ironical - sigh.
-mr. bill
Not that this "asserted" fact will placate the anti-helmet crowd (who assert they aren't) - ever.
Ironical - sigh.
-mr. bill
05-17-16 | 09:45 PM
#2061

Been Around Awhile
Joined: Oct 2004
Posts: 30,679
Likes: 1,989
From: Burlington Iowa
Bikes: Vaterland and Ragazzi
Also, I'd like to see ED visits separated from actual hospitalizations as the 0-14 age group being taken to the hospital says nothing about the severity of the trauma, or indeed if any actually occurred. When you look at the stats for deaths and hospitalizations for kids and young adults, falls aren't the real issue.
Risk analyses without consideration of injury severity are just exercises in blowing smoke.
05-18-16 | 08:27 AM
#2062
Senior Member
Joined: May 2004
Posts: 12,103
Likes: 96
From: Wilmington, DE
Bikes: 2016 Hong Fu FM-079-F, 1984 Trek 660, 2005 Iron Horse Warrior Expert, 2009 Pedal Force CX1, 2016 Islabikes Beinn 20 (son's)
Well "hard" as opposed to "soft" is pretty much a given. Most everything causing an impact or sharp acceleration will have a surface impact. "Flat" possibly refers to sidewalks and roads which are leading locations for falls. Along with residences for which falls are mostly bathroom, may or may not be flat. Or it may be from his helmet researches which do show that impact on flat surfaces are the most likely to result in TBI. I don't know that it's worth arguing about, or the trouble to source.
05-18-16 | 08:57 AM
#2063
Senior Member
Joined: Apr 2011
Posts: 15,278
Likes: 342
From: Alpharetta, GA
Bikes: Nashbar Road
Most residences have stairs. Stairs have little relevance to cycling. Holding up simple falls as the leading cause of TBI and thus heralding the bicycle helmet as the cure without considering why those falls happened (and further posting about it as if the assumption is fact) is a bit misleading, but not surprising. And then there's the whole severity thing.
Please examine his links, or other resources about your objection, more carefully before arguing about them.
05-18-16 | 09:09 AM
#2064
Senior Member
Joined: May 2004
Posts: 12,103
Likes: 96
From: Wilmington, DE
Bikes: 2016 Hong Fu FM-079-F, 1984 Trek 660, 2005 Iron Horse Warrior Expert, 2009 Pedal Force CX1, 2016 Islabikes Beinn 20 (son's)
I believe one of those links Joe posted did break it down to "same-level" falls as opposed to stairs and ladders etc. It might have been a related reference, but IIRC it was one of his. Same level falls were very much more frequent, so your objection is not valid.
Please examine his links, or other resources about your objection, more carefully before arguing about them.
Please examine his links, or other resources about your objection, more carefully before arguing about them.
From the CDC link:
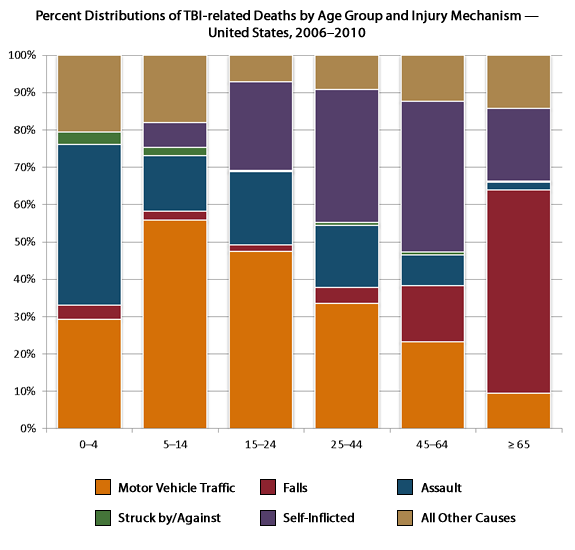
Motor vehicle crashes were the leading cause for children and young adults ages 5-24 years. (Among TBI-related deaths in 2006–2010)
Assaults were the leading cause for children ages 0-4. (Among TBI-related deaths in 2006–2010)
Assaults were the leading cause of TBI-related ED visits for persons 15 to 24 years of age.
Motor vehicle crashes were the leading cause of hospitalizations for adolescents and persons ages 15-44 years.
If you look at this chart and consider the age groups likely to be riding bikes, falls are far from an overwhelming leading cause:
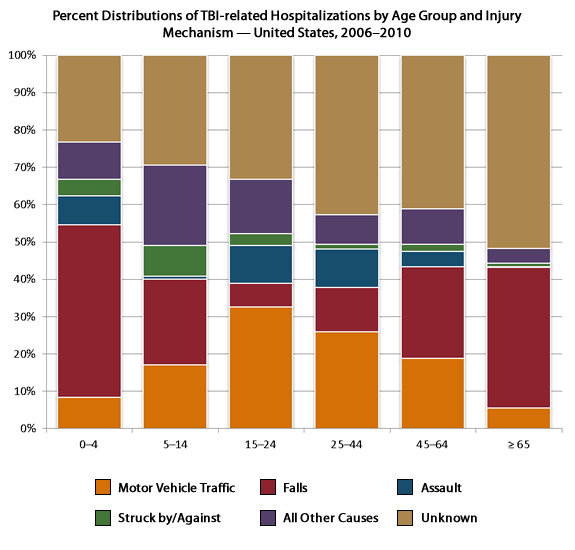
There's a whole lot of 'unknown' in the data (which makes it questionable to begin with) and in the highly active age brackets there's that big orange section.
05-18-16 | 09:34 AM
#2065
Senior Member


Joined: Apr 2009
Posts: 39,897
Likes: 3,865
From: New Rochelle, NY
Bikes: too many bikes from 1967 10s (5x2)Frejus to a Sumitomo Ti/Chorus aluminum 10s (10x2), plus one non-susp mtn bike I use as my commuter
Statistics are almost useless for analysis. There are many subcategories, so most people trying to parse out meaningful data will adjust or compensate trying for greater relevance. Unfortunately, that means that assumptions determine the outcome.
For example, if we look at all the head injuries due to simple falls, we find a large percentage occur among the elderly. Not because the elderly are more prone to head injury, but simply because the elderly tend to fall more often for a variety of reasons. So, we might adjust the numbers to remove all TBIs occurring in nursing homes and hospitals and find that the picture has changed significantly.
We might likewise look at TBI data among bicyclists, and see if there are age group disparities, ie. children or adult over 65. Also, it's hard to get realistic data on actual usage, so even if we accept the raw numbers, we can't compute a rate.
So, while we do know that some bicycle crashes lead to TBIs, we don't have a decent sense of the likelihood, during anyone's lifetime cycling career, or what kinds of riding, ie. urban commuting, sport road riding, are more or less likely to lead to a TBI.
So, IMO, all this debate about the data is pointless, since the numbers can be tweaked any way someone wants.
On the flip side, even though the large percentage of TBIs from simple falls, isn't on point for discussing TBI risk when bicycling, it is relevant from a personal risk assessment. There is a risk, and we can approach it from the point of view of reducing every risk, or frame the relative risk within our other daily risks. Do you accept living near a nuclear reactor, diet/heart disease or cancer, other sports activities, drive a sports car, home with steep stairs, etc.
This is how I made my personal decision about helmets, approaching the decision based on what level of risk I consider acceptable, combined with my expectations/belief about the degree to which a helmet might make a difference.
For example, if we look at all the head injuries due to simple falls, we find a large percentage occur among the elderly. Not because the elderly are more prone to head injury, but simply because the elderly tend to fall more often for a variety of reasons. So, we might adjust the numbers to remove all TBIs occurring in nursing homes and hospitals and find that the picture has changed significantly.
We might likewise look at TBI data among bicyclists, and see if there are age group disparities, ie. children or adult over 65. Also, it's hard to get realistic data on actual usage, so even if we accept the raw numbers, we can't compute a rate.
So, while we do know that some bicycle crashes lead to TBIs, we don't have a decent sense of the likelihood, during anyone's lifetime cycling career, or what kinds of riding, ie. urban commuting, sport road riding, are more or less likely to lead to a TBI.
So, IMO, all this debate about the data is pointless, since the numbers can be tweaked any way someone wants.
On the flip side, even though the large percentage of TBIs from simple falls, isn't on point for discussing TBI risk when bicycling, it is relevant from a personal risk assessment. There is a risk, and we can approach it from the point of view of reducing every risk, or frame the relative risk within our other daily risks. Do you accept living near a nuclear reactor, diet/heart disease or cancer, other sports activities, drive a sports car, home with steep stairs, etc.
This is how I made my personal decision about helmets, approaching the decision based on what level of risk I consider acceptable, combined with my expectations/belief about the degree to which a helmet might make a difference.
__________________
FB
Chain-L site
An ounce of diagnosis is worth a pound of cure.
Just because I'm tired of arguing, doesn't mean you're right.
�One accurate measurement is worth a thousand expert opinions� - Adm Grace Murray Hopper - USN
WARNING, I'm from New York. Thin skinned people should maintain safe distance.
FB
Chain-L site
An ounce of diagnosis is worth a pound of cure.
Just because I'm tired of arguing, doesn't mean you're right.
�One accurate measurement is worth a thousand expert opinions� - Adm Grace Murray Hopper - USN
WARNING, I'm from New York. Thin skinned people should maintain safe distance.
05-18-16 | 09:35 AM
#2066
Senior Member
Joined: Apr 2011
Posts: 15,278
Likes: 342
From: Alpharetta, GA
Bikes: Nashbar Road
...
If you look at this chart and consider the age groups likely to be riding bikes, falls are far from an overwhelming leading cause:
There's a whole lot of 'unknown' in the data (which makes it questionable to begin with) and in the highly active age brackets there's that big orange section.
If you look at this chart and consider the age groups likely to be riding bikes, falls are far from an overwhelming leading cause:
There's a whole lot of 'unknown' in the data (which makes it questionable to begin with) and in the highly active age brackets there's that big orange section.
It's probably better to pick a chart or table that directly illustrates your point or theory, which is (I think) that most TBI's are not the result of falls? Or not on hard flat surfaces? What is the significance of that, if you're right?
05-18-16 | 09:53 AM
#2067
Senior Member
Joined: Apr 2011
Posts: 15,278
Likes: 342
From: Alpharetta, GA
Bikes: Nashbar Road
Exactly.
05-18-16 | 10:22 AM
#2068
Senior Member
Joined: Aug 2010
Posts: 588
Likes: 3
From: Southern California
Bikes: Gary Fisher Hi-Fi Deluxe, Giant Stance, Cannondale Synapse, Diamondback 8sp IGH, 1989 Merckx
Helmet foam:
Styrofoam is and has been the reigning energy absorption material used in helmets. It is cheap, easy to work with, controllable and lasts 20 years or more.
Styrofoam’s effectiveness was established around 1960 at USC (University of Southern California) by Professor Lombard and his successor Professor Hurt.
Their research was sponsored by the US Navy which was looking to reduce the number of severe head injuries to its pilots when they ‘crashed’ onto carrier decks.
Lombard and Hurt were testing differing materials when the Germans accidentally gave them the clue to the answer. They had ordered a quality 35mm camera from Germany (I do not remember the manufacturer). When the camera arrived Professor Hurt, then a grad student, opened the box and found that the camera was cradled in Styrofoam. They then tested Styrofoam and found the answer to their quest.
Since that time, more than a half-century ago, Styrofoam (Expanded Poly Styrene) remains the best proven material to attenuate impact loadings to helmet wearers’ heads. You’ll also find it cradling your new TV, computer, etcetera.
There is no ‘one’ Styrofoam used to make helmet liners. Hemet liner material varies in density. The density, back when I researched the matter, was expressed in pounds-per-cubic-foot. Motorcycle helmet liner foam varied from 1.5 to 3.
The higher the density, the greater the force required to start the brain-saving crushing. In order to meet performance standards, lower density foam had to be thicker so that it would not ‘bottom’ during testing.
The best performance USC’s Head Protection Laboratory found while testing helmets for my article published in Motorcyclist magazine in 1981 was also the cheapest. That helmet used 1.5 pound foam which was about 1.5” thick. It was huge. It cost $40 at K-Mart. Neither company is now in business as far as I know. The Snell helmets gave the highest deceleration numbers while still barely passing the DOT loading and dwell specifications.
Current bicycle helmets use much higher density foam than any motorcycle helmet I am aware off, as high as 6#/cubic foot. This higher density is needed to make-up for the lack of complete coverage dictated by the need for ventilation cutouts. Professor Hurt expressed concern to me about this hardness and wondered, he was by then retired, if threshold (the load that would begin crushing) “g” numbers might be rather high for the then current bicycle helmets (circa 2005). This is a very good question and one that is not easy to answer because helmet testing is now done almost exclusively by manufacturers who, for various reasons, do not share their testing data.
Bicycle helmet liners break and crush. Motorcycle liners just crush. Breaking is not as effective as crushing.
Joe
Styrofoam is and has been the reigning energy absorption material used in helmets. It is cheap, easy to work with, controllable and lasts 20 years or more.
Styrofoam’s effectiveness was established around 1960 at USC (University of Southern California) by Professor Lombard and his successor Professor Hurt.
Their research was sponsored by the US Navy which was looking to reduce the number of severe head injuries to its pilots when they ‘crashed’ onto carrier decks.
Lombard and Hurt were testing differing materials when the Germans accidentally gave them the clue to the answer. They had ordered a quality 35mm camera from Germany (I do not remember the manufacturer). When the camera arrived Professor Hurt, then a grad student, opened the box and found that the camera was cradled in Styrofoam. They then tested Styrofoam and found the answer to their quest.
Since that time, more than a half-century ago, Styrofoam (Expanded Poly Styrene) remains the best proven material to attenuate impact loadings to helmet wearers’ heads. You’ll also find it cradling your new TV, computer, etcetera.
There is no ‘one’ Styrofoam used to make helmet liners. Hemet liner material varies in density. The density, back when I researched the matter, was expressed in pounds-per-cubic-foot. Motorcycle helmet liner foam varied from 1.5 to 3.
The higher the density, the greater the force required to start the brain-saving crushing. In order to meet performance standards, lower density foam had to be thicker so that it would not ‘bottom’ during testing.
The best performance USC’s Head Protection Laboratory found while testing helmets for my article published in Motorcyclist magazine in 1981 was also the cheapest. That helmet used 1.5 pound foam which was about 1.5” thick. It was huge. It cost $40 at K-Mart. Neither company is now in business as far as I know. The Snell helmets gave the highest deceleration numbers while still barely passing the DOT loading and dwell specifications.
Current bicycle helmets use much higher density foam than any motorcycle helmet I am aware off, as high as 6#/cubic foot. This higher density is needed to make-up for the lack of complete coverage dictated by the need for ventilation cutouts. Professor Hurt expressed concern to me about this hardness and wondered, he was by then retired, if threshold (the load that would begin crushing) “g” numbers might be rather high for the then current bicycle helmets (circa 2005). This is a very good question and one that is not easy to answer because helmet testing is now done almost exclusively by manufacturers who, for various reasons, do not share their testing data.
Bicycle helmet liners break and crush. Motorcycle liners just crush. Breaking is not as effective as crushing.
Joe
Last edited by Joe Minton; 05-18-16 at 02:50 PM.
05-18-16 | 10:31 AM
#2069
Senior Member
Joined: May 2004
Posts: 12,103
Likes: 96
From: Wilmington, DE
Bikes: 2016 Hong Fu FM-079-F, 1984 Trek 660, 2005 Iron Horse Warrior Expert, 2009 Pedal Force CX1, 2016 Islabikes Beinn 20 (son's)
You know what's wrong with reasoning from that graph to overall causes of TBI, right? It's not the large "unknown", but consider what it says about the numbers of TBI cases by cause (ie, nothing) and about the non-hospitalized (ER) incidents of TBI (again nothing). The chart shows that injuries from falls are relatively infrequent for the 15-44 age group, but doesn't tell you anything about the aggregate. If there were some absolute numbers in addition to the percentages, it would probably resemble the other chart you saw that had falls accounting for 40.5% of the TBI injuries.
 05-18-16 | 10:43 AM
05-18-16 | 10:43 AM
#2070
Senior Member
Joined: Apr 2009
Posts: 39,897
Likes: 3,865
From: New Rochelle, NY
Bikes: too many bikes from 1967 10s (5x2)Frejus to a Sumitomo Ti/Chorus aluminum 10s (10x2), plus one non-susp mtn bike I use as my commuter
Oops, an error in editing. I meant to say for this purpose, meaning teasing out the relative risk of TBI while bicycling.
__________________
FB
Chain-L site
An ounce of diagnosis is worth a pound of cure.
Just because I'm tired of arguing, doesn't mean you're right.
�One accurate measurement is worth a thousand expert opinions� - Adm Grace Murray Hopper - USN
WARNING, I'm from New York. Thin skinned people should maintain safe distance.
FB
Chain-L site
An ounce of diagnosis is worth a pound of cure.
Just because I'm tired of arguing, doesn't mean you're right.
�One accurate measurement is worth a thousand expert opinions� - Adm Grace Murray Hopper - USN
WARNING, I'm from New York. Thin skinned people should maintain safe distance.
05-18-16 | 12:02 PM
#2071
Senior Member
Joined: Apr 2011
Posts: 15,278
Likes: 342
From: Alpharetta, GA
Bikes: Nashbar Road
That's more like it. We don't have the right kind of data, or the data is problematic when we do find some that would otherwise be useful, to get a definitive answer to that.
05-18-16 | 04:42 PM
#2072
Senior Member
Joined: Aug 2010
Posts: 588
Likes: 3
From: Southern California
Bikes: Gary Fisher Hi-Fi Deluxe, Giant Stance, Cannondale Synapse, Diamondback 8sp IGH, 1989 Merckx
"There are three kinds of lies: Lies, damned lies and statistics." -- Mark Twain. Funny but sometimes true.
When I was researching for my bicycle helmet article (published in Bicycle Rider, spring of 1985/6?) I came to know a doctoral candidate at the University of Illinois @ Chicago (I'm sorry that I have forgotten his name). He was trying to study head injury deaths amongst children. He needed to gather enough information to be able to draw conclusions, make predictions and defend his consequent thesis. His frustration, and mine, was that no one, anywhere in America, seemed to care all that much about the causes of head trauma deaths amongst children. We could find no data bases. None.
We both finally concluded that folks simply considered childhood accidental death to be ‘normal’. By the word “folks” I include ER personnel, investigative police, schools and parents themselves. ‘They’ accepted childhood head trauma deaths as a normal but “to be expected” tragedy. A given; some kids were gonna die.
A majority of these childhood deaths, as far as we could determine, were TBIs.
Statistically meaningful conclusions were simply not possible.
I am not sure that it’s much better now.
Joe
When I was researching for my bicycle helmet article (published in Bicycle Rider, spring of 1985/6?) I came to know a doctoral candidate at the University of Illinois @ Chicago (I'm sorry that I have forgotten his name). He was trying to study head injury deaths amongst children. He needed to gather enough information to be able to draw conclusions, make predictions and defend his consequent thesis. His frustration, and mine, was that no one, anywhere in America, seemed to care all that much about the causes of head trauma deaths amongst children. We could find no data bases. None.
We both finally concluded that folks simply considered childhood accidental death to be ‘normal’. By the word “folks” I include ER personnel, investigative police, schools and parents themselves. ‘They’ accepted childhood head trauma deaths as a normal but “to be expected” tragedy. A given; some kids were gonna die.
A majority of these childhood deaths, as far as we could determine, were TBIs.
Statistically meaningful conclusions were simply not possible.
I am not sure that it’s much better now.
Joe
Last edited by Joe Minton; 05-18-16 at 05:16 PM.
05-19-16 | 09:58 AM
#2073

Senior Member
Joined: Jun 2007
Posts: 7,552
Likes: 135
I looked and found this:
Where did you find the reference to 'hard relatively flat surfaces'? Also, I'd like to see ED visits separated from actual hospitalizations as the 0-14 age group being taken to the hospital says nothing about the severity of the trauma, or indeed if any actually occurred. When you look at the stats for deaths and hospitalizations for kids and young adults, falls aren't the real issue.
Where did you find the reference to 'hard relatively flat surfaces'? Also, I'd like to see ED visits separated from actual hospitalizations as the 0-14 age group being taken to the hospital says nothing about the severity of the trauma, or indeed if any actually occurred. When you look at the stats for deaths and hospitalizations for kids and young adults, falls aren't the real issue.
05-19-16 | 10:07 AM
#2074
Senior Member
Joined: Jun 2007
Posts: 7,552
Likes: 135
The real issue with the undefined "crash" stats and associated statements about relative risk (helmet related or not) often cited by self described bicycling safety experts/advocates is the almost complete absence of any reference to injury severity, as they use metrics that ignore injury severity and tabulate every fall and crash as identical in severity.
Risk analyses without consideration of injury severity are just exercises in blowing smoke.
Risk analyses without consideration of injury severity are just exercises in blowing smoke.
It could also be suggested that less severe injuries are more common than moderate and severe injuries, so helmets are effective in preventing or mitigating the majority of cycling-related TBI.
They're certainly not a panacea for all injury, especially if it does not involve the head (duh), and of doubtful efficacy where total cycling safety is concerned, but helmets do have their place and can be effective in rare circumstances.
05-19-16 | 11:45 AM
#2075

Senior Member
Joined: Jun 2007
Posts: 3,509
Likes: 2
From: SW Ohio
Bikes: 3 good used ones
There was one study posted in one of these thread which did get into detail. It was a recent study -- 2014? '15? -- which looked into the efficacy of helmets regarding injury mitigation for various severity levels of injury. Basic conclusions were that helmets would reduce or eliminate injury by a factor of 10 for minor injury, 5 for moderate injury, and 2 for serious injury. I.e., as the severity of injury increased, effectiveness of helmets to prevent or mitigate injury diminished. I don't think I'm getting the numbers exactly right, but after looking at the study parameters, performance, and conclusions, I don't remember anyone being able to claim it was not legit.
It could also be suggested that less severe injuries are more common than moderate and severe injuries, so helmets are effective in preventing or mitigating the majority of cycling-related TBI.
They're certainly not a panacea for all injury, especially if it does not involve the head (duh), and of doubtful efficacy where total cycling safety is concerned, but helmets do have their place and can be effective in rare circumstances.
It could also be suggested that less severe injuries are more common than moderate and severe injuries, so helmets are effective in preventing or mitigating the majority of cycling-related TBI.
They're certainly not a panacea for all injury, especially if it does not involve the head (duh), and of doubtful efficacy where total cycling safety is concerned, but helmets do have their place and can be effective in rare circumstances.
